I started taking TDF about 4 months ago and my viral load (HBV DNA) has become “undetectable”. Even so, my HBsAg is still high (above 5.000).
I would like to know if there is any possibility of this value decreasing? And if there is a higher risk of developing complications even with “undetectable” HBV DNA due to the high HBsAg value?
And what would be considered a high HBsAg value to be considered a risk factor?
Over time (years) antiviral therapy can reduce the level of HBsAg slightly. I am not entirely sure what the specific risk of complications is between high HBsAg and undetectable DNA, as it’s complicated with all the different phases in hepatitis B.
In any case, the underlying liver damage (fibrosis measured by fibroscan) has much more of an effect on complication risk and this is what your doctors will likely be focusing on.
I’m also asking myself this question because my HBs antigen level is around 50,000 IU, which is very high compared to all the messages I read. I’ve been on entecavir for 7 years and am undetectable. But my antigen level isn’t decreasing.
I also wonder if I’m at higher risk of complications and not eligible for the new treatments that are coming.
Furthermore, I was diagnosed with fibromyalgia about ten years ago, which doctors attribute to my chronic hepatitis.
Hi @Marie_David,
I am not sure about the risks of complications, but I think many chronic patients, myself included, seem to be in a similar situation. With the medications in clinical trials, yes, they start with patients whose surface antigen levels are well below 5000 IU. If they get good and long-lasting results, they can expand to include patients with higher surface antigen levels. That is my understanding of the process. We are not forgotten.
Surface antigen levels move after the 10-year mark, at least in my case. I am in my 11th year of being on treatment, and it was only last year that we noticed a slight reduction in my surface antigen level. We can’t read too much into it, but we shall see what the numbers look like when I get another test later this year. I am not sure this is a general experienece but I would hope so for everyone.
Best, Bansah1
I actually don’t know if there’s any correlation between high surface antigen and risk of liver disease. That’s a very good question.
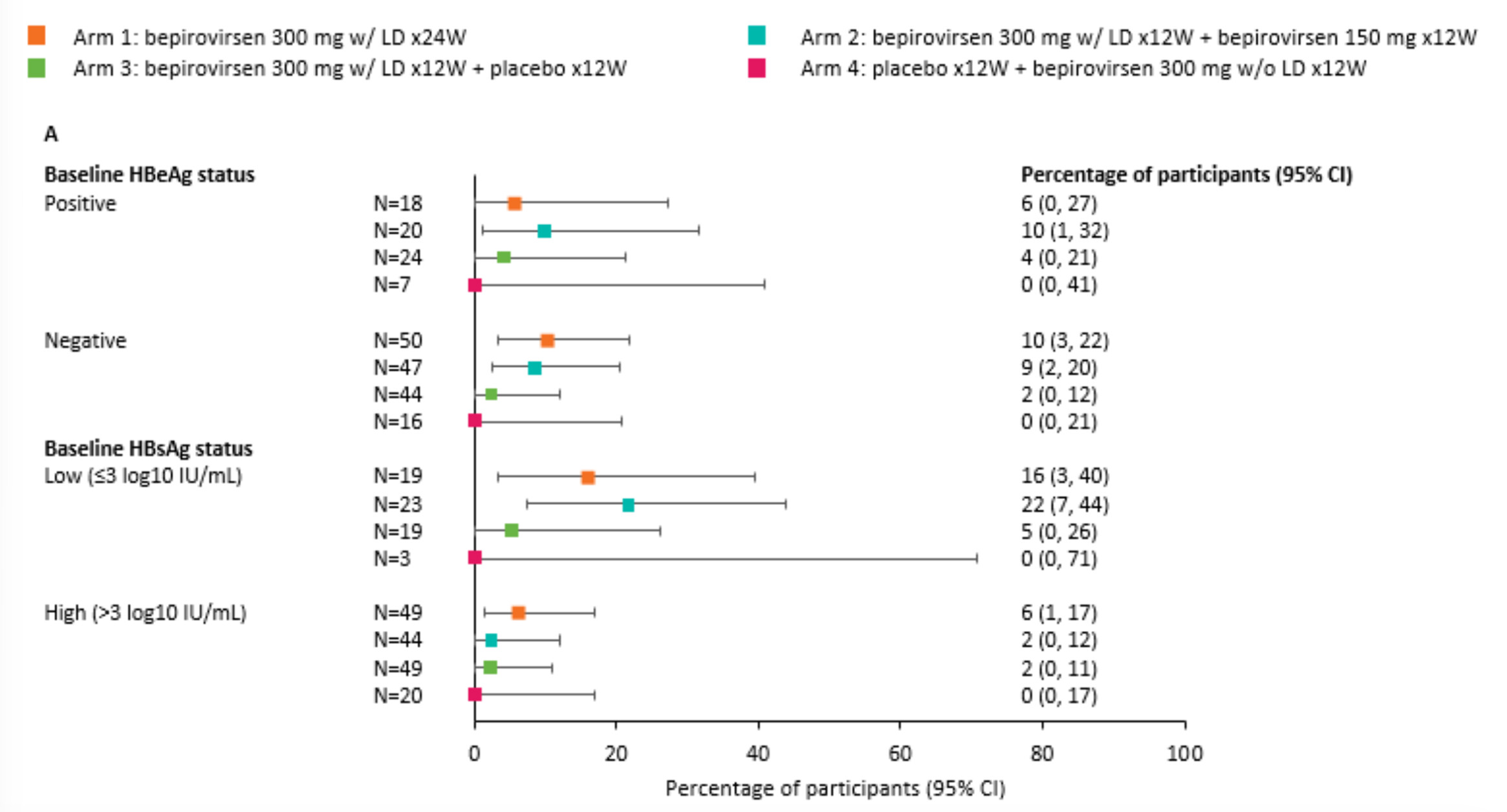
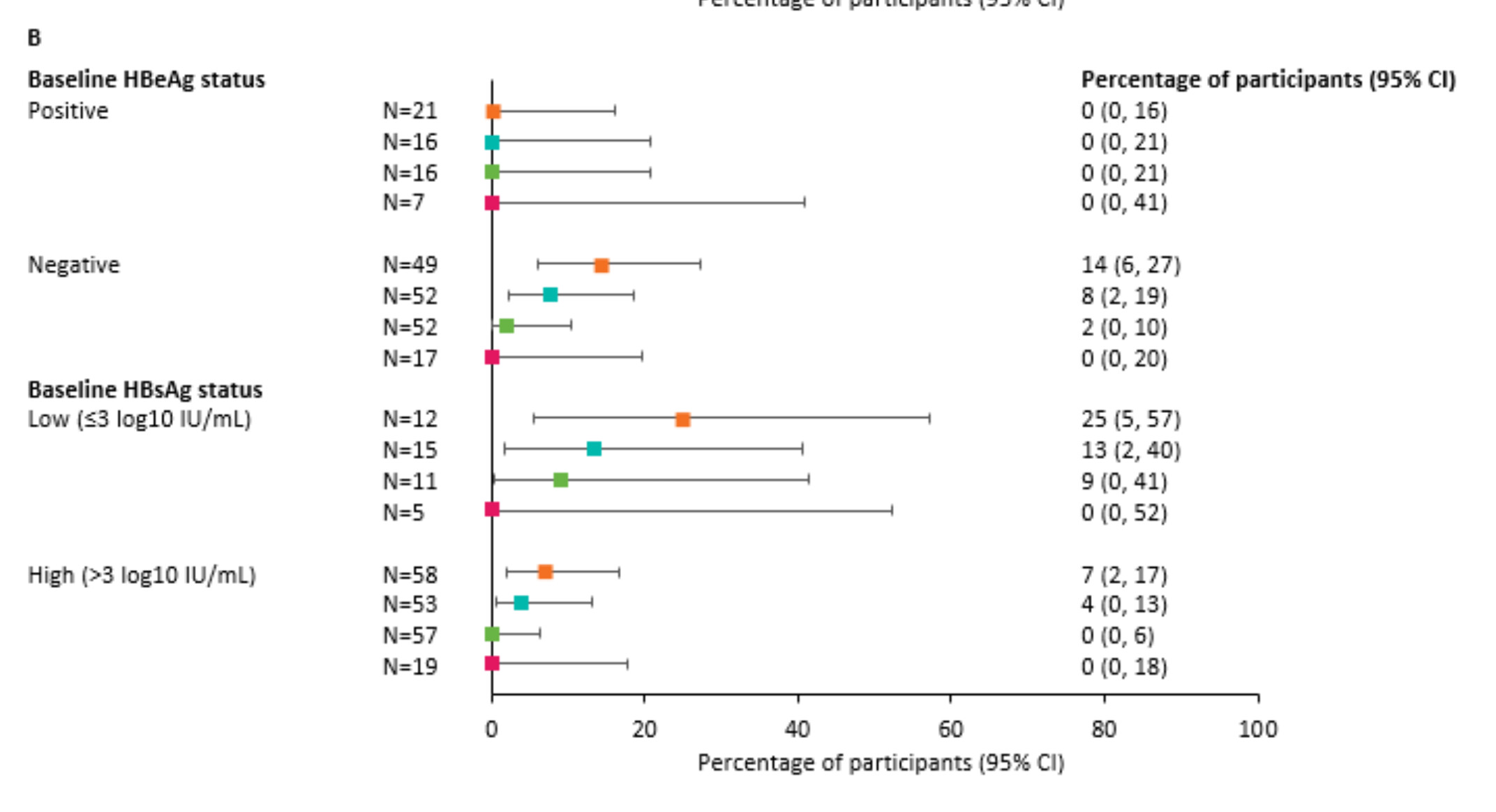
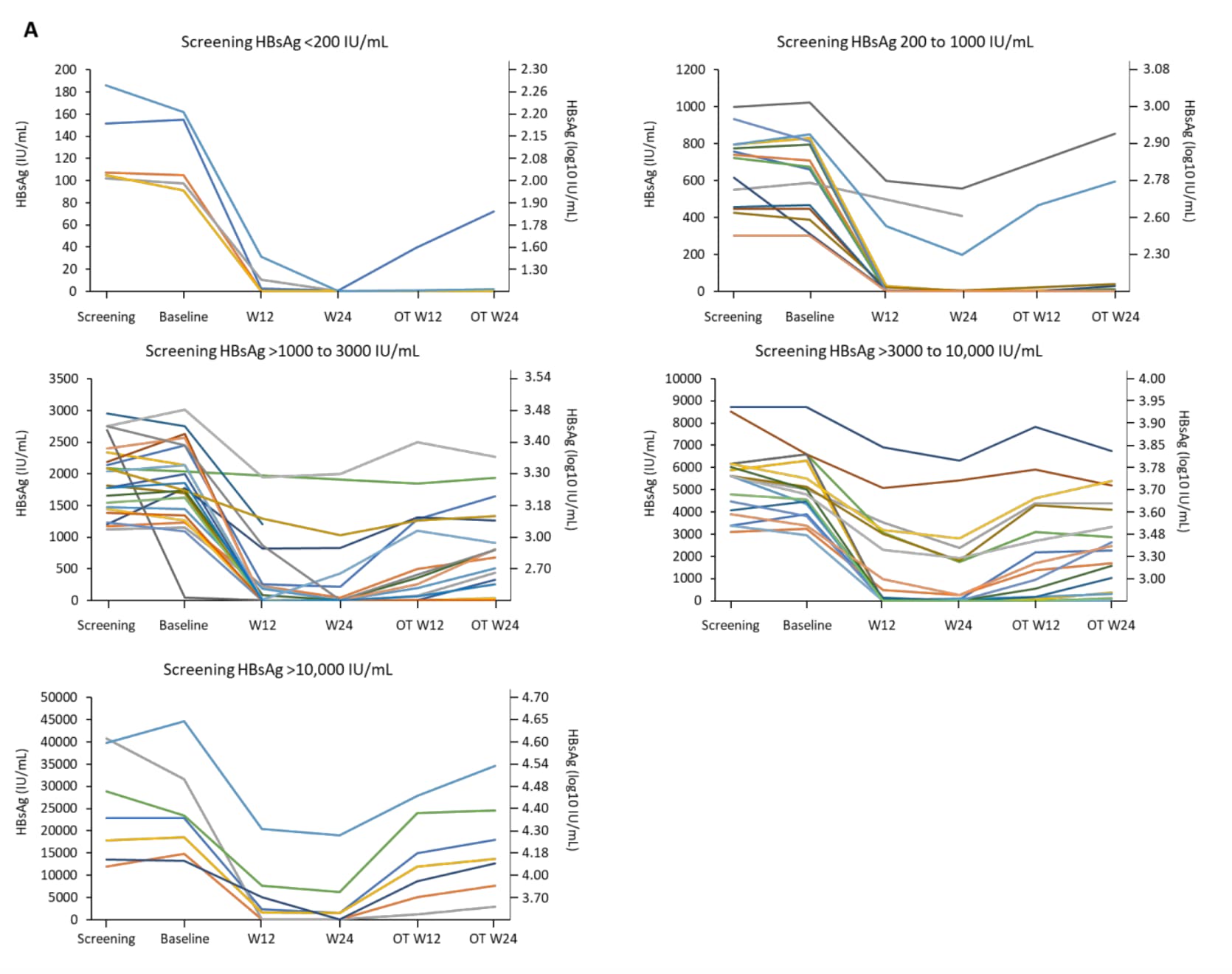
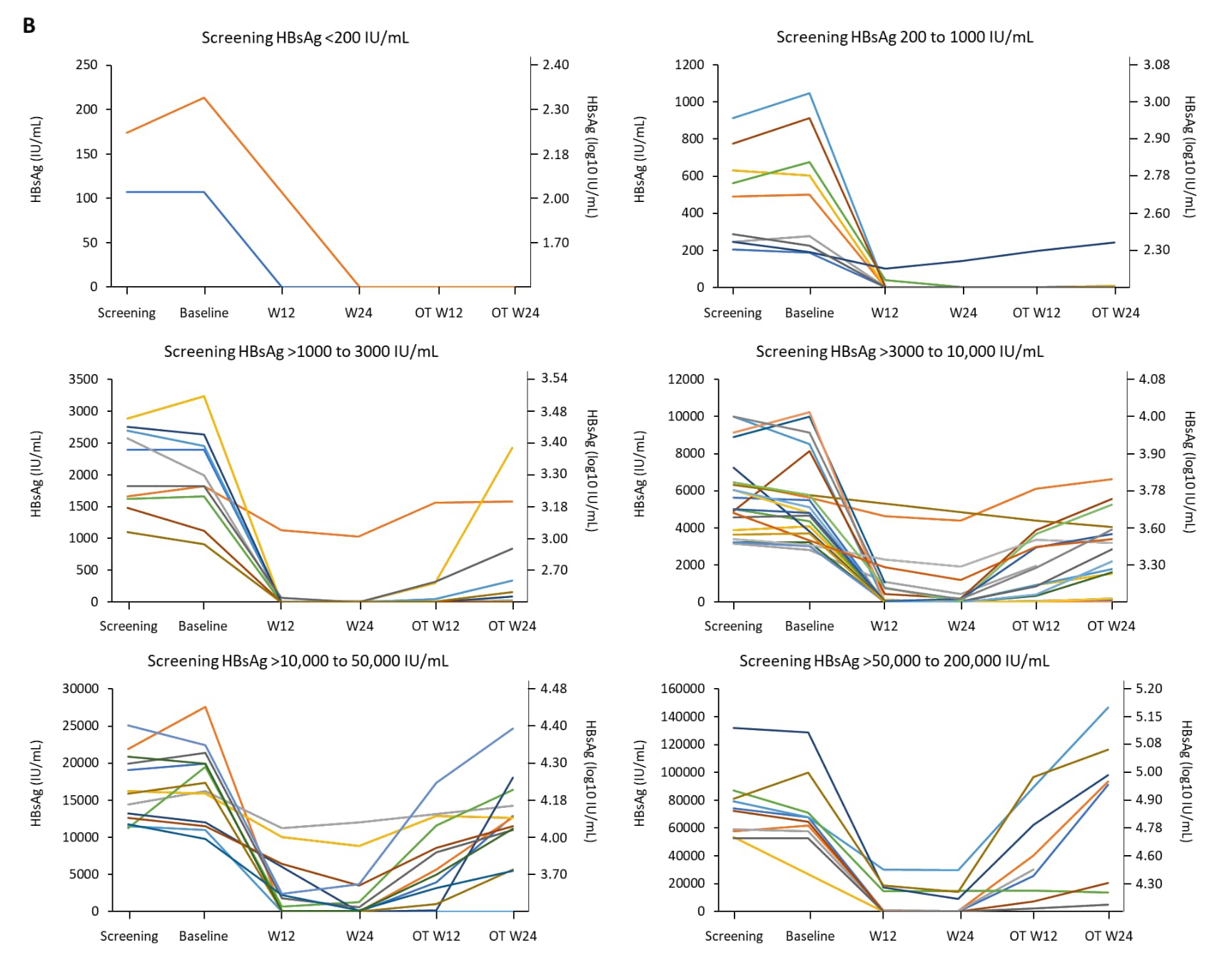
I found this supplementary appendix from the phase II B-Clear study for Bepirovirsen. From the data presented here, it seems clear that people with lower HBsAg are more likely to achieve functional cure.
Here are 2 charts I found showing the % of patients achieving functional cure. The first one (A) shows data for patients on NUCs (tenofovir, entecavir), and the second one (B) is for people not on NUCs.
For those of you who are not math nerds, 3 log10 = 1000
As for myself, I think my trajectory of HBsAg is perhaps kind of atypical. I had a hepatitis flare in 2014 (before I was on treatment), where my ALT went up to 1278, and AST to 500. At the time, my surface antigen was only 241. The doctor got me started on tenofovir, and my HBsAg actually went up after starting medication, and slowly climbed to back over 1000 over the course of the next 3 years. It’s not at all clear to me why. After that, I moved to the United States, and my doctor here didn’t test my surface antigen very often. I was actually trying to get it tested for a while, but the lab kept running the qualitative one (positive/negative) instead of quantitative, even when I specifically told them I wanted quantitative.
Anyways, I had another flare in 2022, much less severe than the one in 2014. I think it’s most likely that my HBsAg started going down again after that flare, because this year, before I started Bepirovirsen, it was in the 400s. I don’t think I’ve met another person whose HBsAg went up while on NUCs yet.
Thank you all for the interaction and clarifications.
That’s precisely my question: I understood here, based on many comments, especially from Dr. @thomastu and Dr. @availlant, that low HBsAg levels imply a good prognosis, and even its loss suggests a “functional cure.” Furthermore, some developed medications are highly effective in patients with HBsAg below 1000 IU/ml.
However, my question is the opposite:
What numbers are considered high for HBsAg?
Does having high HBsAg levels correlate with any prognosis for developing liver disease?
Right, I think I understand why HBsAg loss leads to a better prognosis. But let’s say you have one person with HBsAg 50,000 and another person with 3,000. It’s not clear/obvious to me whether the higher levels of HBs would lead to a more rapid disease progression, assuming both patients are on current first-line treatments.
This is excellent. So there shouldn’t be a correlation. We just need to stick to the treatment to reduce the risks.
Only in my last tests did they quantify my HBsAg. My doctor said that quantifying HBsAg is not common practice in my country… all the “control” and monitoring is done on HBV DNA and the level of fibrosis (by imaging or liver biopsy).
@La.sciamachie I think what I’m saying is that I don’t really know whether there is a correlation or not. Maybe some of the @HealthExperts would. But certainly taking medication as prescribed leads to a better prognosis.
I have no idea what the average HBsAg is. The only way I’m aware of to lower HBsAg are the new drugs in development. We’ve heard the most about bepirovirsen, but there are other drugs in the research pipeline that are designed to lower surface antigen as well.
The question is that the levels of HBsAg is associated with disease progression in CHB patients with NUCs treatment and suppression of HBV DNA .
If we consider only HBsAg which mostly produced from ccc DNA in HBeAg +ve patients and integrated HBV DNA in HBeAg -ve patients , currently, there are no studies on the cut off levels of HBsAg that would disease progression unlike HBV DNA which has the cut off level at > 2,000 IU/ml . this may be due to the fact that.HBsAg it’s not only produced from cccDNA , it can be produced from integrated HBV DNA therefore HBsAg don’t vary with the phases of CHB as HBV DNA level.
For HBeAg +ve CHB patients, there will be an increase in transcriptional activity of cccDNA leading to increase inHBV DNA level meanwhile increasing HBsAg at the same time. When the body immune system need to eliminate.HBV results in necroinflammatory processes need to fibrosis with scarring formation, cirrhosis and HCC.in CHB patients who are not taking antiviral drug. High HBsAg levels not the direct cause of.necroinflammatory processes, rather it is the high HBV DNA level that caused chronic liver injury and HBV DNA integration. This is consistent with previous studies about HBsAg levels and disease outcomes in CHB patients without antiviral therapy. However, CHB patients with NUCs treatment and have high HBsAg levels and undetectable HBV DNA may have reduce risk of cirrhosis and HCC but can’t complete eliminate risk to zero .
If we consider HBsAg is not carcinogenic , there may be other factors that contribute to cirrhosis and HCC in these patients . In the past, research studies about CHB patients taking antiviral drugs might not control some confounding factors such as MASLD , obesity,alcohol , smoking, lifestyle of patients , aflatoxin exposure etc that may affect the outcome about fibrosis, cirrhosis and HCC. Therefore, it would be appropriate to conduct the research to answer the question about impact of high HBsAg levels and disease outcomes in CHB patients with NUCs completely HBV DNA suppression. I hope this may help you.
Thanks for these questions and I’ll attempt to answer as best as I can.
This depends on what you are considering. There are high levels for if a particular person is likely to clear their infection (for example after treatment cessation, or using these new therapies). It is generally accepted that this number is around 100IU/mL - Any higher than this and your chances of clearing the infection are lower.
There are not really high levels to consider if someone is at risk of liver disease - HBsAg doesn’t really correlate with liver disease in most circumstances.
There are new therapies that can lower HBsAg levels (e.g., DAP/TOM and other siRNA approaches), but I am not aware of any other lifestyle modifications that can lower HBsAg levels.
My hbsag got as low 1.77 u/ml at the end of the treatment period. But bounced back to 10.94 u/ml 6 months post treatment. My hbeag ended at .96 u/ml eot, eventually ended at .73 u/ml 6 months post treatment.
NGL while I am grateful, I can understand the interferon treatment can be challenging for alot people including myself. But if my hbsag continue to remain low(touch wood), perhaps it would be worthwhile to try and find a way, and go on the treatment again. As I understand it the vir 3434 played a role, if I am correct as an artificial form of the antibody. I recall my hbsag went to 7.71 u/ml after the first week of treatment. So I was fortunate I responded to the treatment.
It perhaps it is worth mentioning my wbc was still just below the acceptable range at about the end of post treatment. I’m hoping that my wbc recovers to the level prior to treatment.
Of course I will need to consult with my doctor. Just wondering what you do if you were in my shoes?.
I’m curious how long it has been since the trial ended, and whether you’ve had any more HBsAg testing done since then. The bad news is that it’s unlikely that you would be able to try VIR-3434 again, unless it’s approved by the FDA and becomes available on the open market. If Vir takes that drug to phase III trials, I’m almost certain that people who have gotten the drug already in earlier phase clinical trials would not be eligible (based on what I’ve seen with the inclusion criteria with many other HBV drug trials).
On the other hand, the good news is that if you have a sustained partial response (e.g. HBsAg stays under 100 for an extended period of time), you actually have a decent chance of clearing it on your own in the next several years. Also, participating in the VIR-3434 trial would not necessarily exclude you from other drug trials, especially if the next trial is testing a different class of drug than the one you received in the Vir trial.
Welcome to the forum and thanks for sharing your experiences. It’s great to hear that you had such a strong decrease in your HBsAg levels. Indeed Vir3434 is a modified anti-HBs antibody.
Indeed, it is worth talking to your doctor about what is available. We do know that people with lower HBsAg levels also respond better with interferon therapy, which you could potentially discuss with your doctor.