My name is Dee and I’m new to the forum, and super thankful for it.
I was diagnosed with CHB in 2013, and my viral load has been relatively low, so I haven’t been place on any treatments.
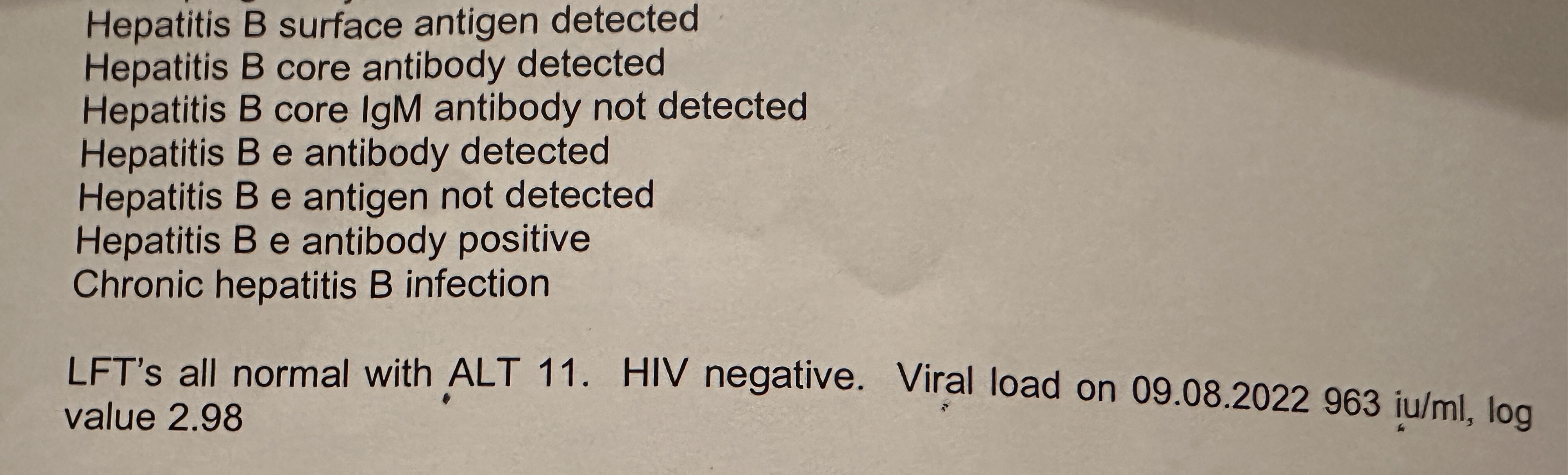
I recently had a baby, and I had routine scans and tests during pregnancy to monitor my viral load. I was told that I didn’t need any medication going into my 3rd trimester due to my low VL (please see the image).
Here’s my worry, my baby didn’t get the vaccine immediately, even though I kept asking for it and challenging. Vaccine was administered the next day (within 24hrs) after several arguments with the hospital staff.
I have since challenged this and it’s being investigated, but my liver consultant said the chances of transmission is very low due to my low viral load, and also due to the fact that I had a Cesarean Section.
My child has received all the help b vaccine, just waiting to get the 12 months, then get tested.
I’m so worried and each time I think about it, I’m said and anxious because I feel like I may have hurt my child.
Is the consultant right, or have I just been told this to calm my nerves?
Thanks for your question and sorry to hear about the stress you’ve been under. It’s also really frustrating that your requests were not responded to.
However, indeed, the risk of transmission is quite low due to your low viral load. Infants who have been given birth dose (defined as within 24 hours of birth) are adequately protected. See figure 2 in this WHO report (page 29 of the PDF https://apps.who.int/iris/bitstream/handle/10665/333391/9789240002708-eng.pdf). It shows that maternal virus levels less than 20000 do not result in a chronic infection in newborns, who are very highly susceptible to chronic infection.
I completely understand your fear. However, your baby was vaccinated within 24 hours and should be well protected especially that your viral level is low. I have 3 kids, and I was always worried if any of them got infected during the birth. However, they were all checked when they turned 1 and they were all good. So I totally understand your fear, because I went through that fear with every of my child.
I have a few questions as a new mom of a 8-day old baby boy.
I just gave birth on the 13th of March 2024 and fortunately, the hospital had given HBIg and Hep B 1st dose to my baby within 24 hours. My doctor suggested me to breastfeed. I’ve been doing it for 8 days as of 21 March 2024. However, I have noticed that my nipples are cracked and sometimes I can see red spots (due to bleeding, I think). Is there a chance of transmission of hep b virus to my baby via cracked and bleeding nipples? My current status: HbsAg 5.47 IU/ml as of 7 March 2024 and HBV DNA 50 IU/ml as of 4 Dec 2023. My baby only received HBIg and Hep B first dose.
Hello, I was breastfeeding normally all three kids. However, when I had a broken skin on my nipples I waited when it healed up, and I was pumping the milk from that breast until it was healed up. Use the lanolin it helps with healing or there is also egyptian magic cream that is very good for healing quickly.
Hi @ThomasTu
I have a similar question to those on this thread. I am 8 months pregnant and have chronic hep B. I have and have always had low viral loads (currently <20 UI HBV/ml). I am Australian but will give birth in a country where only the hep B vaccine is given to babies of hep B positive mothers within 24 hours of birth. A shot of immunoglobulin is not provided. My questions are: (1) What are the risks of not providing immunoglobulin to my baby? I’m asking to know how much I should advocate to my health care providers (2) Can I start to breastfeed before my baby receives the hep B vaccine? (3) should I temporarily stop breastfeeding if my nipples are cracked or bleeding ? Appreciate your help!
My viral load is 7417 at june 6 th 2025 ,in pregnant women my doctor gave me Tenofovir AF 25 mg,as you replied maternal virus less than 20,000 do not result in chronic infection in newborn ,should I start using the medicine I also fear of antivirals withdrawal will make the condition worst so want to know should I use r not please Reply sir very much worried from 15 days , unable to sleep atleast because of this fear
Decisions regarding postpartum continuation of NA therapy depend on multiple factors. If a mother plans another pregnancy, had a preexisting treatment indication (e.g. chronic hepatitis or fibrosis), or wishes to continue therapy, treatment should be maintained.
In the case where treatment is stopped (as was the management guidelines before), then ongoing monitoring is generally offered. This allows any changes (such as ALT flares and inflammation) to be detected quickly and you would be offered treatment before any irreversible damage occurs.
Hi @ Harini
In HBsAg +ve pregnant women, if the initial visit assessments show that the patient is eligible with treatment criteria then TDF/TAF can be started early .
In your case, I think that your doctor has started TAF because you may had preexisting treatment indications eg: chronic hepatitis ( HBV DNA > 2,000 IU/ml and ALT > UNL or 40 IU/ml ) , fibrosis ( APRI > 0.5 / Fibroscan (LSM) > 7 kPa ) as @ Thomas Tu mentioned in EASL guidelines May 2025 .
If pregnant women with HBsAg +ve don’t meet the treatment criteria, TDF/ TAF prophylaxis must be considered in cases with HBV DNA > 200,000 IU/ml or HBeAg + ve and start at 28 weeks of gestational age until delivery or complete HBV vaccination series (0,1,6) within 6 months after delivery.
After stopping TDF/TAF , ALT levels should be closely and continuously monitored at least 6 months. Hepatitis flare is diagnosed relies on serum ALT > 2-3 times of UNL . Most of serum ALT levels in hepatitis flares that occur after stopping TDF/TAF usually < 5 times of UNL and severe hepatitis leading to liver failure is rarely occurs.
chul_chan
Chulapong Chanta MD. Pediatrics