So one or two years ago the doctor advised me to take medication for life, I wasn’t too keen about this, so I just stayed away for one or two years, and here I am posting this, haven’t experienced any health issues yet. So makes me wonder do we really have to take medication ? Should we just wait untill we really get sick ? I have read the viral load can fluctuate naturally without medication, guess the immune system trying to suppress the virus itself. Will do a viral load test, I am curious what the results will be.
First, you never “have to” take a medication. It is always at the individual’s preference.
The current HBV treatment guidelines call for treating people with a substantial risk of having ongoing progressive liver disease. The guidelines typically rely on having a combination of high viral replication level and elevated liver enzymes, but they are complex and vary somewhat in the different regions of the world. Their common feature is that clinical and epidemiological studies clearly indicate that starting treatment in those folks provides significant health benefits. Liver enzymes typically normalize and the rate of progression to liver fibrosis, cirrhosis, and liver cancer is greatly slowed after starting treatment.
Note that it is quite possible for liver enzymes to be pretty high without the person feeling symptoms. The liver has an enormous extra capacity to do its job, particularly in younger and healthier people, so damage can be ongoing without a person feeling ill. High liver enzymes indicate that damage is ongoing, and the damage is cumulative over time.
The current front-line drugs, entecavir and 2 types of tenofovir, are very safe in almost everyone, so side effects are not normally a big problem. Some of the HBV+ people on this forum can chime in with their personal experiences.
Taking drugs for life is certainly no fun. I have asthma, high blood pressure and high cholesterol, so I’m on a few drugs that I have to take daily and will have to do so for life. That can be expensive depending on where a person lives and what their insurance system is. However, in each case, my doctor has made the decision based on her decades of experience that the benefits to me from taking the drugs are much higher than the side effects from doing so. That is the same judgement your physician has made. I recommend discussing your hesitancy with her/him to see why the recommendation to start therapy was made. That will help you make a decision you feel comfortable with.
My ALT and AST levels were normal in the range for many years, let’s say 10 years or so, couldn’t measure viral load because not available in my country back then, now it is possible, so for viral load I have let’s say 4 measurements in the last 3-4 years.
Hi @hepb1,
That is an interesting question. I just want to add to what @john.tavis have said. Aside from the clinical guidelines which John has touched on, I believe one’s family history of liver cancer might warrant them to start treatment. Some patients actually have a history of multiple family members or just a family member dying from liver cancer and many providers will want to start treatment in situations like that.
Additionally, patients belonging to certain ethnic groups have a higher likelihood/chance to develop liver cancer very early than other ethnic groups. It is known that being African or of an a African descent puts one at an early risk of developing liver cancer. Here too a provider might want to treat a patient based on this history.
Finally, sometimes the patient do not want to take any risk by waiting and they request to start treatment. Here too a provider might start treatment.
These are all unique situations under which treatment becomes necessary. Not everyone fits in here, hence the importance of having a conversation about treatment with a provider. You do not want to wait until your liver is severely damaged or has failed or developed a cancer before you start treatment as that might not be helpful at that point. I hope you continue to remain monitored by your provider, very crucial and vital with this virus. Because things can get worse without any warning or signs/symptoms. Being seen frequently by your provider, getting blood work and ultrasound done are the way to go if you do not want to start treatment.
I hope this in addition to John’s response is helpful. Best, Bansah1.
There have been fantastic answers to your queries so far. Just to reiterate: your liver can be injured without you knowing because it doesn’t have any nerves. Many times, the first symptoms of Hepatitis B are from liver failure or liver cancer, when it’s too late to do anything.
You are in the fortunate position to know that you have Hep B, have insight into what kind of risk you have of liver disease, and catch it early enough to prevent any progression with medication. It is, as @john.tavis mentions, your choice with your doctor as to whether you take medications or not. But it’s important to be thankful that you are being provided that choice, as many others are not in such a position (only 10% of people with hep B know they have it, walking around with this preventable cancer risk but no awareness to stop it).
The best practice is to make sure you’re being monitored with the recommended tests and, if indicated by the results, consider treatment given the risk involved.
Your answers are very clear and insightful, thank you for them.
I just want to add one thing regarding the reluctance of starting the antiviral medication, since I’ve been reluctant myself about starting it.
So in my case the biggest fear is not that once I’m starting taking the medicine it will be probably for life. But the actual fear is that I’d be starting with a present medicine for my CHB, which would prevent future meds from doing their job at full potential and cure the disease.
It’s not a fear based on any readings or actual knowledge, mostly it’s just an assumption and maybe even a bit of paranoia. But it’s something always present as a thought in the back of my mind, keeping me away from actually start taking Entecavir.
So I want to ask you: is it absurd as a thought that something like that might happen? Or is it, at least in theory, possible for a current antiviral medicine to come in conflict with a future one aiming for a functional cure or even real cure?
Great question, @Mihai_P! As far as I can see, patients on antiviral therapy are considered in pretty much all upcoming curative therapies, some trials even requiring that patients have been on antiviral therapy for several years. I would not expect that taking on antiviral treatment now would stop you from being considered from any cures that scientists find in the future.
Thomas is exactly correct. All clinical trials now being performed with experimental drugs for HBV will enroll patients who are currently taking any of the three main oral antiviral medications (ETV, TDF or TAF). These new medications in developent will be added to these oral antiviral medications in combination. In some trials, participants may have to switch the medication they are taking (i.e. switching from ETV to TDF) but this will have no impact on the viral suppression they maintain.
To be honest what you’re saying makes total sense and I would expect a lower (or even undetected) viral load to be better for future medications that are aiming for reducing the HBsAg values.
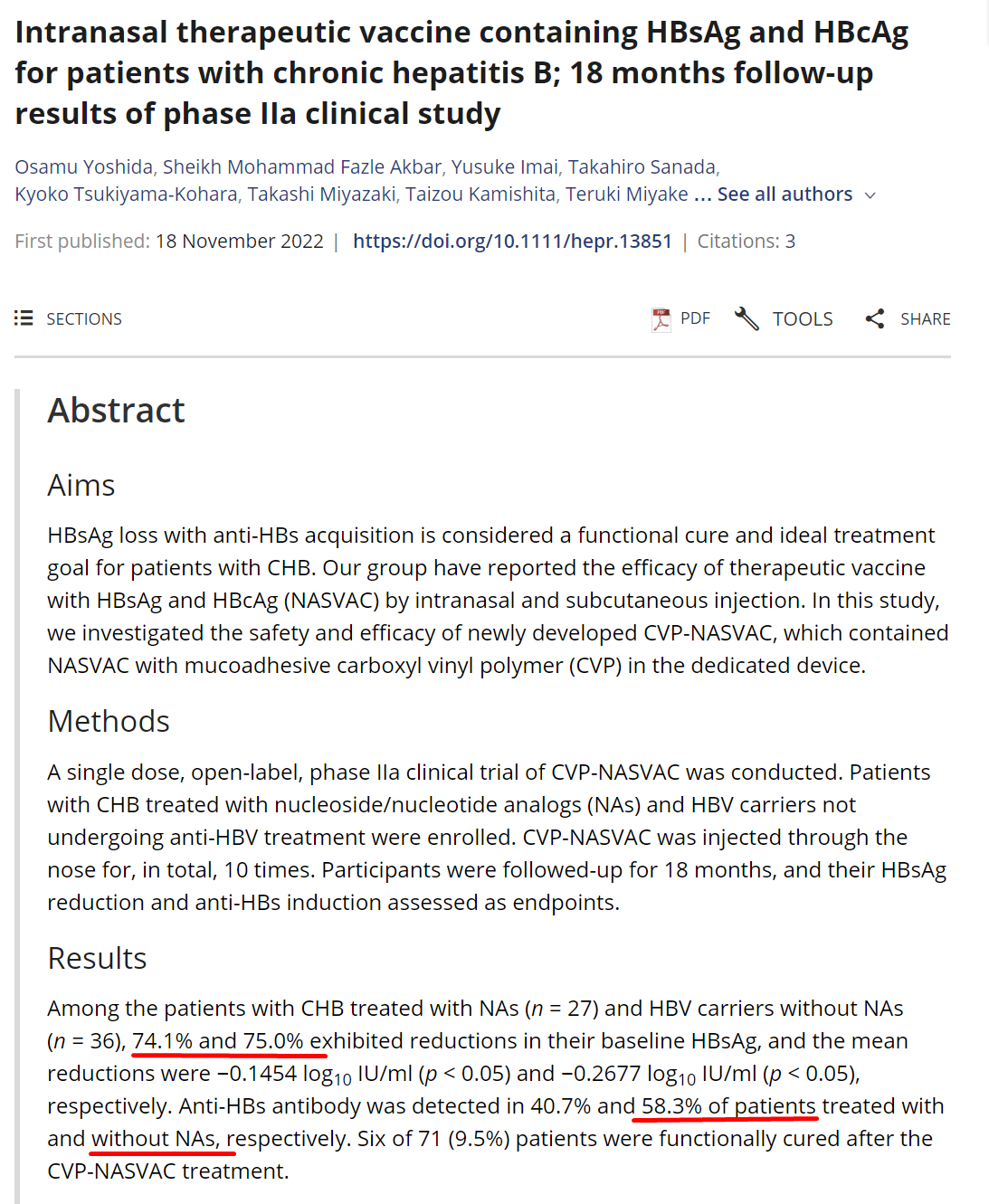
I guess one of the articles that I’ve read and raised some concerns was the one in the link below, especially the parts marked with read in the screenshot attached, where you can see that the percentage of better results were in the category of patient not being under any NUC treatment.
So it look as if CVP-NASVAC would work a bit better for ones not being under antivirals, or I’m understanding the article wrong?
I fully agree with Andrews and Thomas. The chance that taking a nucleoside analog such as Tenofovir or Entecavir rendering you permanently poorly responsive to a new medication is vanishingly small. As Andrew points out, Nucs are actually a component of a great many of the combination trials that are ongoing in search of a functional cure.
So you have uncovered a curious oddity with HBV: in some very restrictive cases, viral activity can actually be associated with improved antiviral responses. These examples are limited to immunotherapies like pegylated interferon and NASVAC.
In these cases, viral replication results in hepatocytes producing larger amounts of the viral antigens associated specifically with viral replication (HBeAg, HBcAg and related antigens we call HBcrAg). If hepatocytes are expressing these agents actively, they can be more easily targeted by agents stimulating immune function against HBV (that target HBeAg and or HBcAg).
However, remember that this is not the case for HBsAg (which comes from cells with integrated HBV DNA which do not make HBeAg or HBcAg). Here HBsAg is equally abundant in the presence or absence of NUCs. Thus, while antiviral response might be marginally better in these specific cases, over all HBsAg loss (and functional) is still as rare as during NUC therapy.