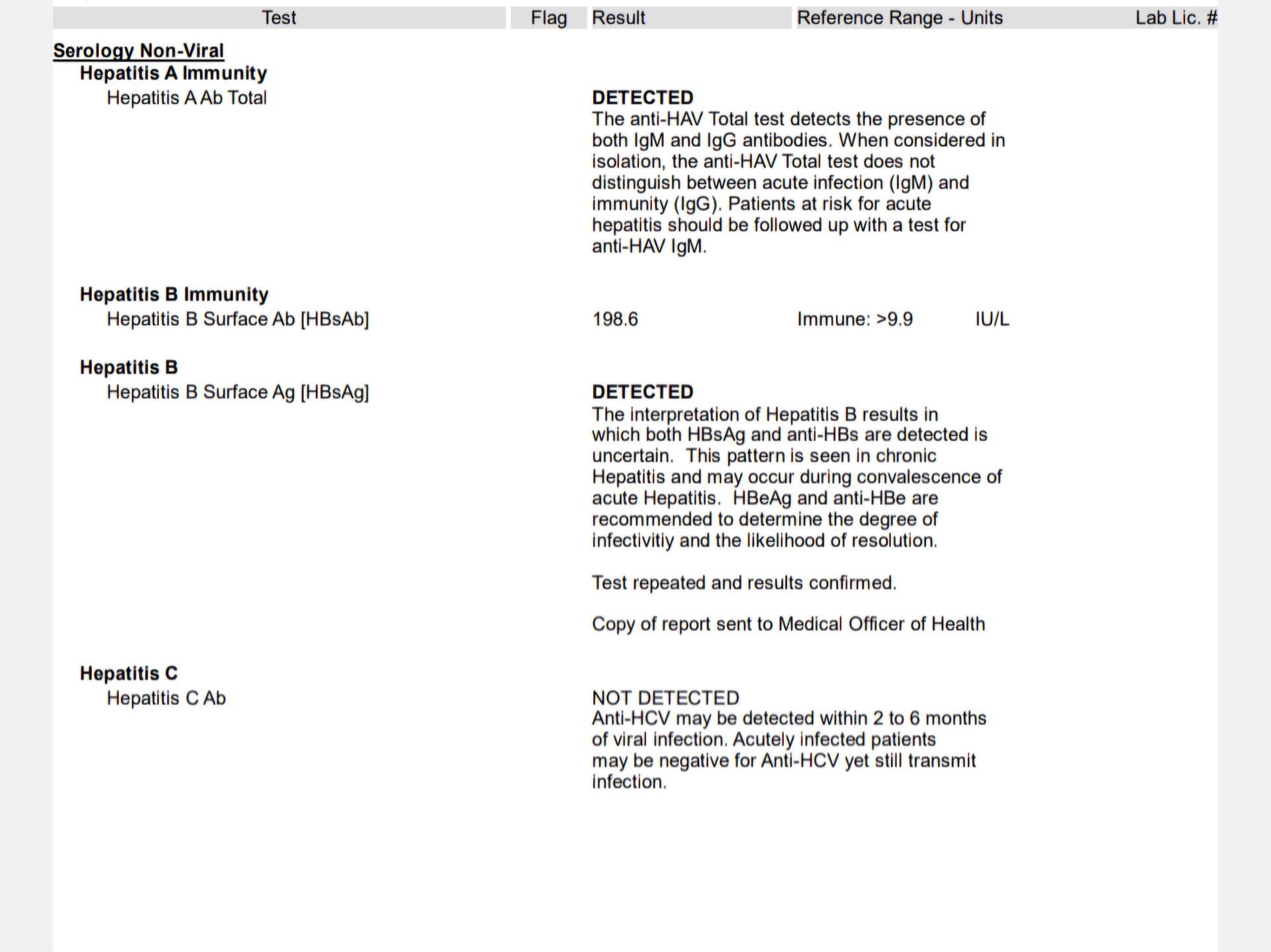
Hepatitis B Surface Ab [HBsAb] 74.8 IU/L
As a chronic carrier with HBsAg positive, what is the importance of the antibodies and why does my doctor test for it every year?
Hepatitis B Surface Ab [HBsAb] 74.8 IU/L
As a chronic carrier with HBsAg positive, what is the importance of the antibodies and why does my doctor test for it every year?
Dear @Walenat,
This is a great question. The co-positivity of HBsAg and anti-HBs is rare, but is described in the literature (e.g., Long-term outcomes of HBsAg/anti-HBs double-positive versus HBsAg single-positive patients with chronic hepatitis B | Scientific Reports). It appears that people with these results are more likely to seroconvert to HBs-loss, which is a functional cure. It is possible that your doctor is continuing to test for this event, which would mean much less monitoring in the future as well as very good prospects for your health.
Hope this helps,
Thomas
Thank you for the detailed response
it worries me that rising antibodies in the case of chronic hbv can both be hopeful and scary as it says that it also increases the chances of hcc.
I only had antibodies around 9iu/ml in 2020 (I am assuming that they had just started to appear around this time) and rose to about 40iu/ml in 2022 but my doctor has just checked them again and my latest reading is 95iu/ml in 2025. Im not sure what this means… do i have a mutant strain running wild?
I asked him to also run a quantitative Hbsag. Pending results
That’s absolutely right. It increases the chances by 3 fold. But some other studies indicate that it is more dangerous on thoss with Heb eAg negative and those with high HBV viral load and high HBsAg
From what I have read, it seems we are dealing with mutants strain which the antibodies cannot suppress. However, because my HBV fluctuates between detected and undetectable, and all other liver functions tests are okay, I hope that the antiviral is doing a good job. We can only hope.
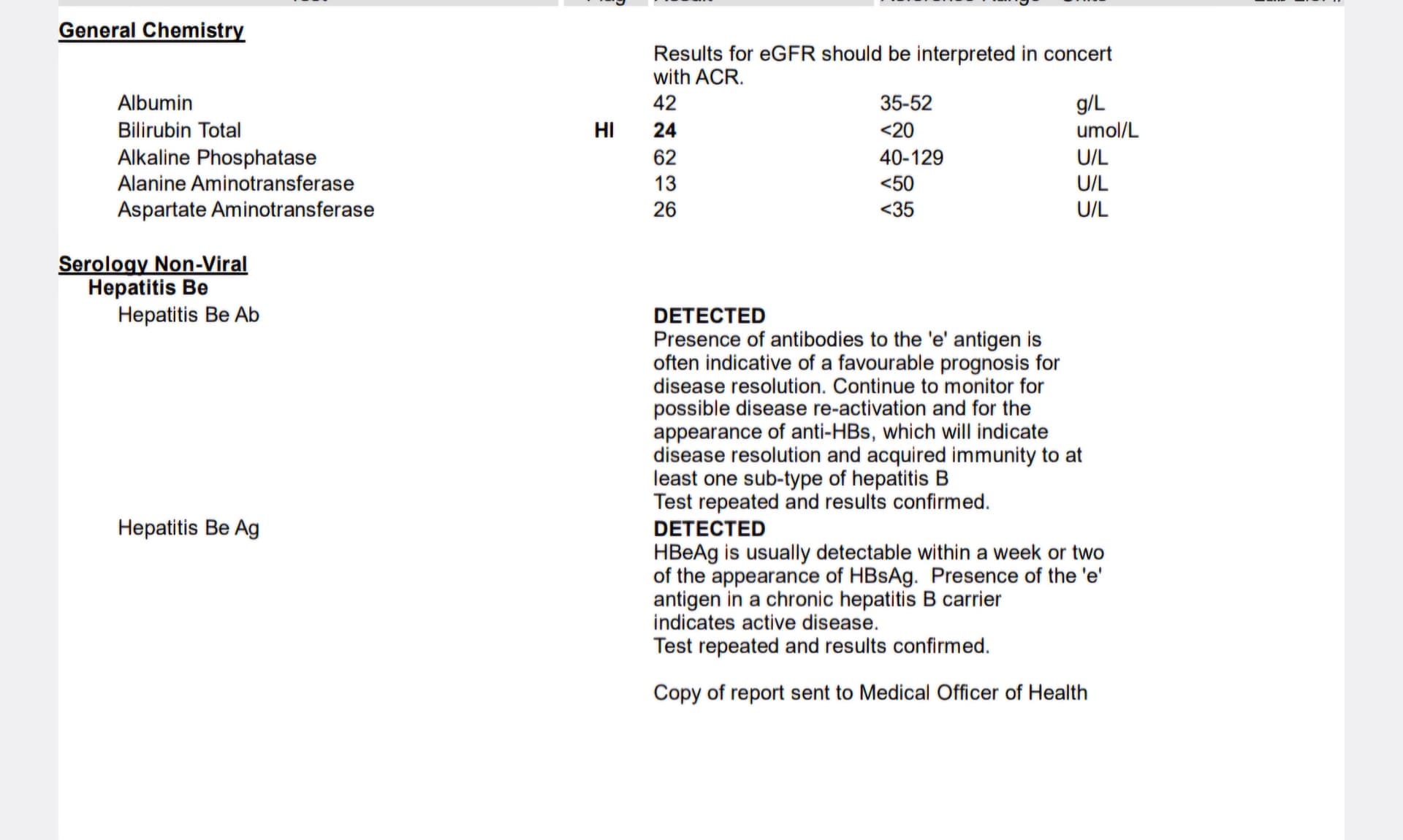
I started antivrial in 2014 and I have been positive for both HBsAg and HbsAb since 2018. Over 200 then and it has reduced to over 70 now. Also, positive for both Heb eAg and Heb eAb. We are dealing with a complicated virus and we can only be hopeful for a functional care.
Oh that’s interesting , I didn’t know you could test positive for both Hbeag and Hbeab at the same time.
I’m Hbeag negative , not on treatment yet as my viral load tends to stay at around 20-60iu/ml.
I’m going to ask to go on treatment as I’ve been reading about the accumulation risk of DNA integrations.
That was eight years ago
I looked it up and it says you may have been in transition from positive to negative and temporarily been positive for both. I wonder if you were to run the Hbeag test again if it would now show negative.
The detection of dual-positivity for both hepatitis B e antigen and hepatitis B e antibody (DEP) is not typically performed for CHB patients. To date, relevant researches have pointed out that the prevalence of DEP is 0.2–2.6% in CHB cases and 10.4% in CHB cases in the immune-active phase (I-AP).3–5 It has been speculated that during the transition between positivity for HBeAg and positivity for anti-HBe, the serologic markers might achieve an optimal rate, making them simultaneously detectable.
The goal seems to have low HBV DNA level and low value of HbsAb when in co positive.
This may be helpful:
" Particularly, by comparing to patients with HBsAg alone, patients with the ‘High’ HBsAg / ‘High’ anti-HBs and ‘Low’ HBsAg / ‘High’ anti-HBs exhibited significantly higher risk for HCC. In the cohort study, survival analysis was used to identify the causal association by a long-term follow-up cohort. However, high HBV load (HBV DNA ≥2000 IU/mL) in CHB patients suggested active viral replication, which was considered as the driving force of disease progression.22,23 Patients with low HBV load had minimal risk of HCC originally. It might explain the reason why coexistence of HBsAg and anti-HBs did not increase risk of HCC, compared to HBsAg alone in CHB patients with low HBV load. Overall, presence of anti-HBs and HBsAg suggested an ongoing immune response which was insufficient to control the chronic HBV infection. The continuous interaction of immune response and viral replication led to chronic inflammation, which is an acknowledged mechanism contributing to the development of HCC. Therefore, in our study, coexistence of HBsAg and anti-HBs was a factor associated with HCC development in CHB patients with high HBV load. However, in patients with high HBV load, only the serological pattern of ‘Low’ HBsAg/‘High’ anti-HBs, but not ‘High’ HBsAg/ ‘High’ anti-HBs, was associated with increased risk of HCC, which was mainly attributed to the hypothesis discussed below."
That’s reassuring, thanks for showing me!
I just got my quantitative Hbsag back, 20,000iu/ml … no seroconversion anytime soon ha ![]()