Hi everyone! My name is Gabriela and I’m an honours student under Thomas Tu. This year I’ve been doing some work on Integrated DNA to better understand its behaviour and help guide future treatment.
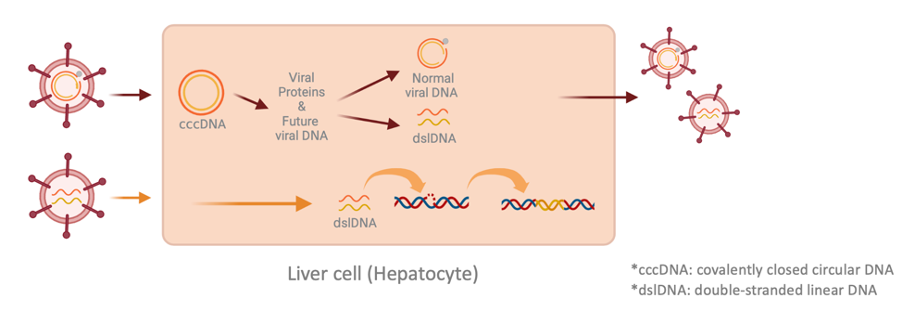
Integrated DNA is a by-product of the virus’s replication cycle. When the virus is replicating, its viral DNA gets transformed into the well-known cccDNA*. This cccDNA serves as a blueprint for the production of all viral proteins and future virus DNA. Intriguingly, a small portion of this future viral DNA is referred to as dslDNA*. In rare instances, it can jump into our cell’s DNA if it is damaged or undergoing replication/repair. The good thing is research has revealed that this integrated DNA has lost parts of itself, rendering it incapable of producing new viruses.
However, what continues to intrigue scientists is the reported link to cancer and the virus’s ability to persist in the body. One study revealed that 85-90% of tumour samples associated with HBV had integrations. On the other hand, research from our lab has shown that integrations usually happen early on during infection, while liver cancer typically occurs decades later. Thus, the apparent link between integrations and cancer can be compared to the chicken-or-egg paradox. Some scientists suggest that integrations may “seem” more frequent in cancer cells, because these cells were already more susceptible to DNA damage, which could lead to integrations.

Additionally, integrations have kept their ability to produce a specific protein called the surface antigen, which is found on the surface of the virus and used to detect HBV infection. This extra source of protein complicates HBV treatment. As clearing the surface protein reduces the risk of liver cancer and can stop or even reverse liver damage. High levels of surface protein also weaken the immune response to the virus. This was shown when scientists used a clever technique to turn down surface protein in mice, and it led to a stronger immune response that could clear the virus.
This means, that integrations may be contributing to both cancer and viral persistence. However, there is still much debate and controversy around how strong this link is, as they occur so rarely and current methods that mimic integrations are lacking in accuracy and numbers.
To combat this shortcoming, our lab has founded a new way to isolate integrations that resemble a natural infection process. To summarise the model: we used a special form of the Hepatitis B virus to infect liver cells. This virus has been modified to carry a gene that makes the infected liver cells resistant to a drug called Zeocin. Here’s where it gets interesting: by treating the cells with Zeocin, we can handpick only the cells that have integrated viral DNA. All other forms of viral DNA are lost as the cells continue to divide.
In total, we have created a range of 138 different cells with integrations in them and will be looking at how they are different to original cells without integrations. This characterisation process will help us to better understand the behaviour of integrations so that we can develop improved ways to treat it.
Thanks for reading and happy to take questions!