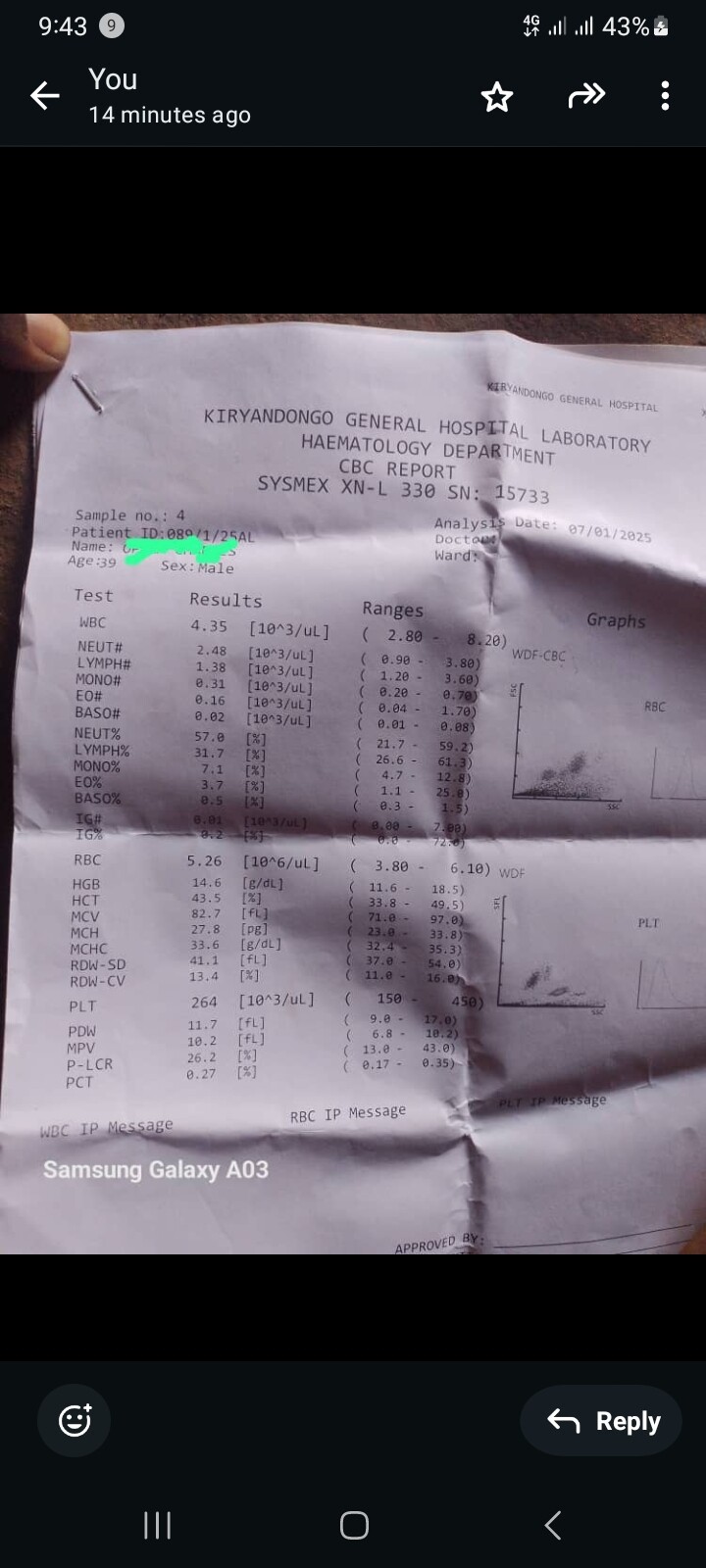
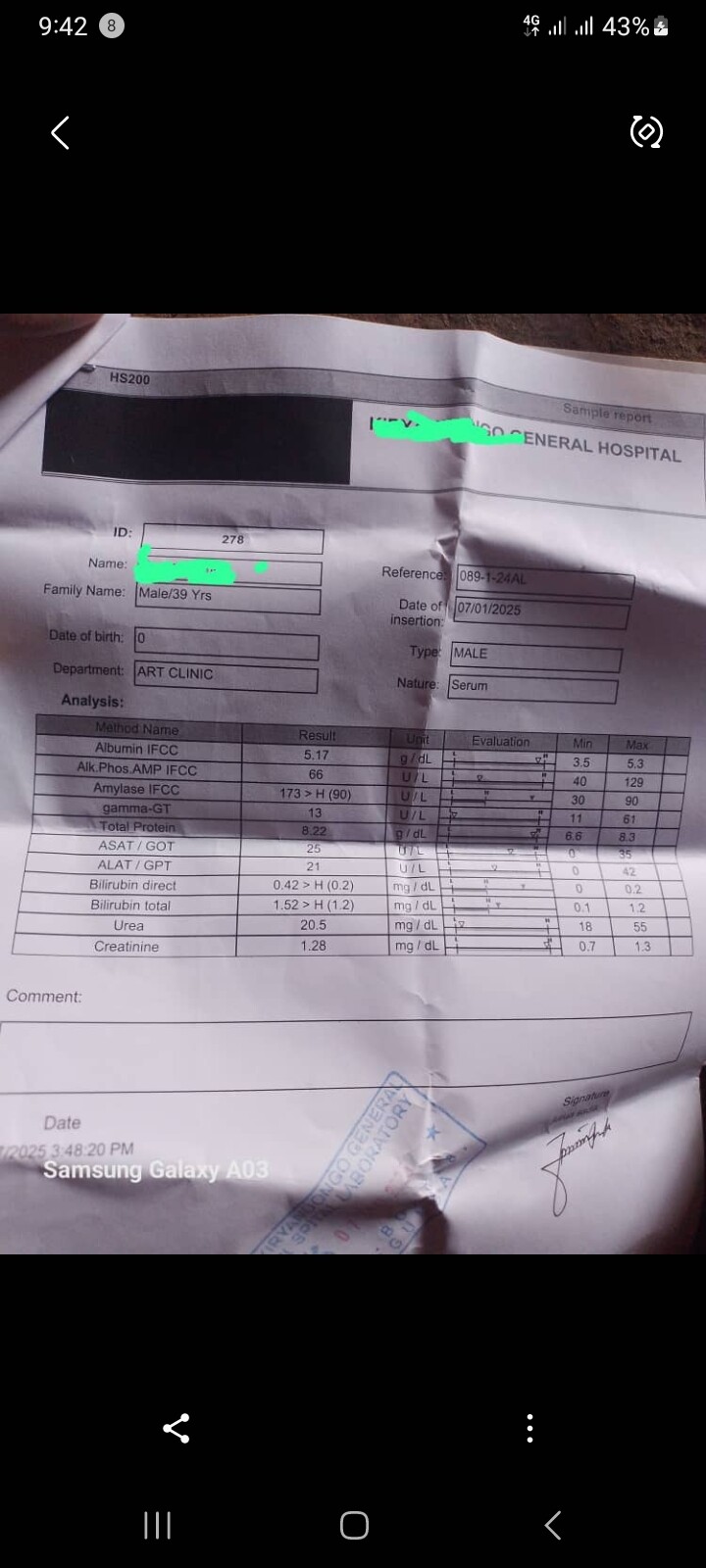
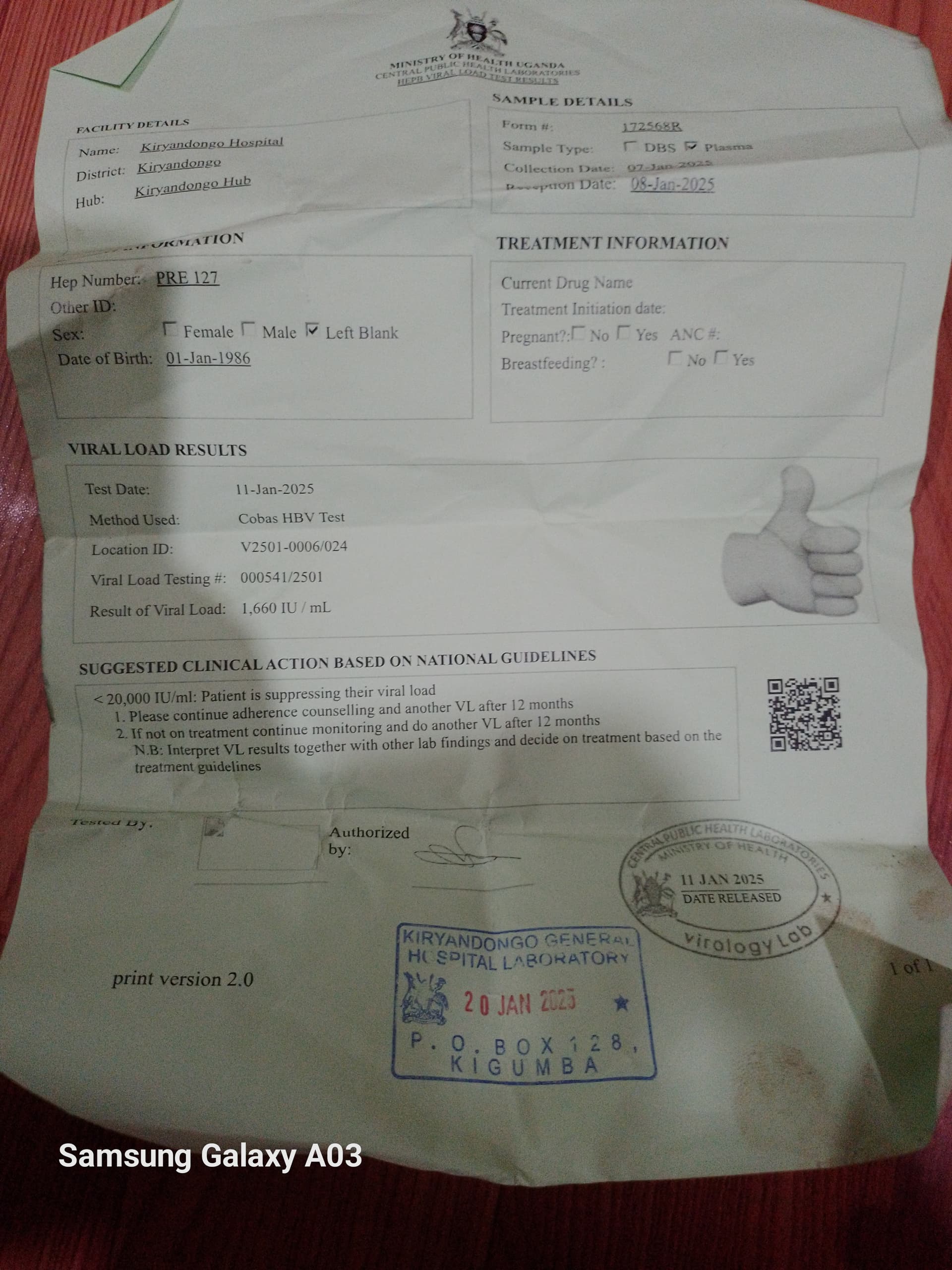
Kindly help me understand my results after the last 6 months
Dear @Opa,
The answer is a bit more nuanced. While there are some people who can develop liver disease progression while at low viral loads, in most cases there are other causes that drive it (e.g. fatty liver, HDV infection, etc.). In these other cases, there are generally indications that there is ongoing liver injury (e.g., increased ALT).
This small increase could still represent the natural flucuations in someone in HBeAg-negative immune control, it should not be framed as something that is deadly or rapid.
Hope this helps,
Thomas
2 Likes
Hello, dear @ThomasTu
Following this conversation, I came up with some questions that may have already been answered in another forum thread, but if you could kindly help me, I would really appreciate it:
-
are the means of monitoring prescribed in current protocols (blood tests and liver imaging every six months) sufficient for the adequate diagnosis of a possible progression of liver disease? Is it possible to have liver disease progression with normal alt and ast laboratory tests and with fibrosis less than grade 2? Is this treatment protocol really safe for everyone?
-
Why is the treatment protocol not modified for treatment as soon as the chronicity of hepatitis B is diagnosed? In my country, Brazil, even with the most recent update, my doctor will only prescribe me antiviral medication after there has been proven progression of the disease and some damage to my liver… even though I have had a liver biopsy and have also been diagnosed with . MASH (grade 1) I do not have access to treatment for virus b. I think it is somehow unfair not to immediately maintain control of the virus to avoid further damage.
1 Like
Hi @La.sciamachie,
Thanks for these great questions.
For most people with no other liver diseases other than hepatitis B, low HBV DNA and normal ALTs means the progression of liver disease is low. The guidelines for liver monitoring have been developed using data from clinical trials. With these trials, the main way to see when antivirals are useful or not has been to measure rates of death, cancer, or disease progression. However, these are averages, and indeed there are cases where disease progression does occur with normal ALT results.
The offering of treatment in many countries is also dictated by whether health systems/insurance will cover the cost of them. This is determined by cost-benefit analysis (how much it costs vs. how much good it does for the person taking it). Again, in the majority of these cases average liver disease progression is used to determine these benefits - using the same clinical trials as above.
I personally believe that there are other reasons people would choose to take antivirals (e.g., to limit their anxiety over disease progression and liver cancer, limiting fear over passing it on, the fact that the reduction of risk of cancer may not be realised until many decades later as is therefore not measurable by clinical trials, etc.) and some scientists/clinicians (some of whom are on this site) are pushing for broadening the number of people who should be offered treatment.
This advocacy is strengthened any time someone on this forum talks about this issue. Part of the reason for starting this forum is not only support for people living with the condition, but also so I (and others) can be exposed to what people in the affected community are going through. This makes it possible for me and others to amplify your voice when I am advocating and talking to the sector (other scientists, clinicians, policy makers, etc.). So I encourage you all to make some noise here so that we can make change happen!
I’d welcome the input from the @ScienceExperts and @HealthExperts involved in these discussions and give your feedback about treatment guidelines.
Hope this helps,
Thomas
4 Likes
I enthusiastically agree with Thomas! I feel that in many cases the current treatment guidelines do not consider many issues of concern to the affected community. Also, they completely fail to consider the limitations to the clinical trial data upon which the guidelines are based. I echo his call to “make some noise”! The HBV community has been ignored for much too long.
John
5 Likes
Hi @ Thomas Tu
Thank you for your valuable answers and I absolutely agree with you.
In my opinion, CHB is a dynamic and complex disease that the clinical course can change overtime and unpredictable. In some situations, to treat or not to treat CHB is a controversial issues, especially if it is in the gray zone (HBV DNA and ALT are discordant) . It depends on the judgment of the clinician to make the decision about when to start treatment and follow with national guidelines.
In some country, China , every CHB patients age > 30 yr who have HBsAg +ve and HBV DNA detectable Were treated with antiviral drug. This is the national policy and has cost effectiveness for HBV horizontally transmission elimination to prevent long-term complications, such as cirrhosis and liver cancer .
If we use evidence based medicine (EBM) to consider and decide when and who to treat. There are 3 important factors to be taken into considerations . The first one is the best available research evidence that support our decision. The second one is clinical expertise of the doctor, which depends on experience in caring CHB patients. The last one which is crucial for the success of the treatment are patient values and expectation. Doctor should explain the risk and benefit of the treatment to the patient in order to take part in the decision to receive treatment or not.
In the past 30 years ago , Interferon is the only drug to use for treatment of CHB patients with serious side effects and many patients often refuse treatment because they can’t tolerate this side effect . At present , oral antiviral drugs with high barrier of resistance have been used to treat CHB patients, however, the patient must take it regularly for the rest of life or until HBV cure occurs.
Most HBV patients are worried about developing liver cancer in the future. These things make some patient lack of self confidence and reduce the full body potential and performances. They don’t want to be followed up and blood drawn for laboratory test frequently due to asymptomatic health condition. Holistic and empathetic approach to the patients are necessary.
In my experience, I used to be CHB patient with immune active phase at 25years old of age during 1992 . At that time there was only interferon based therapy but I don’t want to be treated due to the highly side effects like chemotherapy. I used exercises to boost my immune systems about 2years and HBeAg became seroconversion and turned into inactive carrier in 1994(HBsAg+ve, HBeAg-ve , normal ALT, HBV DNA not available) . I intend to receive treatment due to fluctuations of HBV DNA (normal ALT)during past 10 years ago and consult with hepatologist and suggested to wait and see. Until WHO guidelines and strategiesfor hepatitis elimination has launched about 2016 ,the threshold for treatment of CHB have changed with expansion criteria and I decided to get TAF with out hesitation until now which made me have a better quality of life.
Under circumstances or clinical settings that we can’t differentiate between true inactive carriers (HBsAg< 1,000 , normal ALT , HBV DNA<2,000 ) from asymptomatic CHB infection ( gray zone) , I think that start treatment may have benefits than follow up . It can reduce viral load and HBV integration especially in gray zone CHB patients to prevent liver cancer in the long term .Recent study showed that treatment with true inactive carriers may lead to functional cure after 3 years of therapy and no hepatitis flare after stop antiviral drug. This may be due to the fact that cccDNA in these true inactive carriers are inactive and silent with body immune control and have minimal viral replication, so after stopping treatment with antiviral, there was no effect on cccDNA. https://search.app/6EcdjP6T32wTwUuB7
I hope that this may clarify about some rational of treatment in CHB patients.
chul_chan
Chulapong Chanta MD. Pediatric
5 Likes
Some points supporting treating everyone with hepatitis B
• The treatment is safe, cheap and significantly reduces the risk of people with hepatitis B getting cancer
• Hepatitis B is largely asymptomatic – the infection is really easy to ignore while you live your life and forget to get monitored.
• Being monitored is annoying, and easy to put off. Hospitals are mostly unfriendly institutions built for clinicians and not patients, monitoring takes time and money (even just for taking time off work and parking), you have to fit into hospital and clinicians schedule, and most of the time results in doctors saying you’re fine
• There are psychological issues –everyday you will be reminded that you have an infection, but taking the pill means that you can do something about it.
• For most people it will be lifelong treatment – and this is an issue for everyone with a chronic health condition. Making sure you have access to the treatment will become an issue
• Treating everyone with hepatitis B changes hepatitis B from a transmissible viral infection to a chronic treatable health condition – it has the possibility of reducing stigma.
• It transforms what has been for many people a generational tragedy
• I had hepatitis C – I got cured – this didn’t change much but changed everything –that nagging feeling in the back of my head about liver cancer developing stopped. It’s not huge, but it feels wonderful
• I’m not sure if there is agreement among clinicians if people who use treatment, need to be monitored – and I’m interested to hear ideas about this
• Too many people are dying as a result of hepatitis B – and these deaths are avoidable
6 Likes
Hi @ 1984
I absolutely agree with your fantastic and great point of views about HBV management in CHB patients.
Antiviral drugs are safely and easily to take only one pill a day with minimal side effects. These are game changing and life saving drugs that benefit for curable HCV and treatable HBV.
Antiviral therapy in CHB will relieve patients anxiety about the uncertainty of clinical progression of disease and decrease stigma and discrimination, it will also eliminate the need for frequent blood monitoring which interferes with daily life activities.
Finally, I think we should treat asymptomatic CHB patients as infectious diseases like HIV , TB(LTBI) not as liver disease and anyone with CHB who want to be treated should receive long term treatment as prevention under supervision by clinician.
chul_chan
Chulapong Chanta. MD. Pediatric
4 Likes
Thank you very much for responding to us, Dr. @ThomasTu !
This is the noise we can make, within the possibilities that stigma sometimes tries to imprison us… and we count on all the experts who know how much suffering the B virus can cause to people who are not undergoing treatment.
I, in fact, never understood why we are not treated as soon as the chronicity of the disease is diagnosed. I thought the reason would be for us to lose current medications thinking about possible mutations of the virus and here in this forum I discovered that there is no possibility of loss of effectiveness of the antivirals used.
I may be wrong, but if I had the possibility of making a mistake by acting rather than making a mistake without acting, I would prefer to act and take medication, in order to avoid the greatest damage.
I sincerely hope that the treatment recommendation will be updated again and, this time, expanded to all chronic hepatitis B carriers.
4 Likes
Hello, I am in Shanghai, China, and I am an “inactive HBsAg carrier”. After reading your and other people’s opinions, I am also considering whether I should take medication (my previous doctor suggested that I do not need medication)
Dear @FUMING,
The recent Chinese guidelines are quite permissive and suggest treatment for most people. This includes people with detectable serum HBV DNA, regardless of HBV DNA or ALT levels, and:
A. family history of liver cancer or cirrhosis;
B. age > 30 years;
C. evidence of significant necroinflammation (≥ G2) or fibrosis (≥ F2).
Or, detectable serum HBV DNA and ALT>ULN in the absence of other aetiologies.
It is unclear from what you have provided whether you fit into these categories, but it is worth thinking about and working with a clinician to determine if you would benefit from treatment.
3 Likes
I will communicate with my doctor at my next routine hepatitis B test, thank you very much.
2 Likes
Hey, @ThomasTu @availlant
I have hbsag levels of 1350 rn and I am mostly a genotype D rest of my alt and dna levels are within what youd define an inactive carrier as but why is my hbsag level so high ive read that hbsag levels of >1000 Iu/Ml increases risk of HCC in inactive carriers
What does this mean and should I start my antivirals to reduce the risk or just keep monitoring because my doc asked me to keep monitoring ofc i did not raise this issue with him yet
Thanks!
Dear @void,
Actually, the average HBsAg level in patients is ~10,000 IU/mL so your level is not so high.
Increased risk of liver cancer actually comes from accumulation of new HBV DNA integration events over time so the amount of active HBV replication (HBV DNA) in the blood is proportional to the extent of new integrations.
HBsAg is a derived from cccDNA and integrated HBV DNA so its ability to act as a direct quantitative correlate for HCC risk is doubtful.
However, HCC risk is lower in inactive carriers like yourself (who have low level viral replication). HBsAg levels in inactive carriers tend to be lower (most likely becuase partial immune control of infection, including HBsAg production from cccDNA and integrated HBV DNA, has been established).
That being said, your dilemma about starting therapy or not is one faced by many. We know that starring NUC therapy after age 50 does not have an appreciable effect on HCC risk (becuase of continuing integration). This is why many in the field are considering introduction of NUC therapy before the onset of liver disease (such as in China), which has a better effect in lowering HCC risk. You should discuss this treatment option with your physician.
5 Likes
Hello @ScienceExperts
Thank you so much @availlant for your response.
Ive been monitoring my hbv dna levels and my hbsag levels
24th June 2024
Hbv dna ~500 iu/ml
Hbsag 1150 iu/ml
In November 2024
Hbv dna 396 iu/ml
Hbsag 1356 iu/ml
3rd march 2025
Hbv dna 216 iu/ml
Hbsag >1000 iu/ml (couldnt get the actual number)
This shows while my hbv dna is being controller and suppressed my hbsag isnt and i think it might have risen again so i want to know does this mean have there been more hbv dna integrations in my genome so much so that this is causing hbsag to increase?
And if so doesnt many integarted sites increase my risk of liver disease progression?
Because Ive read in studies like Reach B if you are an inactive carrier but have hbsag >1000 iu/ml your risk is 13.7x times more then a normal inactive carrier…
Ive been pondering and its been stressful lately because i cannot seem to control hbsag and it going up just makes me nervous and lowers any hope of me qualifying for any of the unicorn patient medicines for the future as well as my risk of progression also increases because i am technically an inactive carrier with proper alt and ast and low to no fibrosis so i am not on any meds either.
Hi @void
Please do not read too much into these small changes in your HBsAg levels. These values can fluxuate due to a very large number of variables, and the net change is really not large. They may well go down a little the next time they are measured.
John.
1 Like
Dear @void,
John has it exactly correct. Do no read anything into these very small variations in HBsAg levels.
NUC suppression of HBV DNA (on therapy) is an important and well documented clinical outcome shown to prevent progression of liver disease. While on NUC therapy you should ignore HBsAg (unless it declines to undetectable levels and remains there for 6 months on therapy).
Remember that inactive carriers are NOT receiving antiviral therapy - this is a very different scenario than someone who is on NUC therapy.
1 Like
Thank You @john.tavis and @availlant for your quick replies
But I am not on NUC and I always make sure to keep a check of my values. While researching a bit on HBsAg values, I found that if all my other values and HBV DNA are normal and HBeAg negative while having >1000 HBsAg, it could lead to a very high chance of
Dear @void,
Based on your results in the absence of therapy, it appears that you have partial cure (inactive HBV). A normal ALT result would confirm this.
You risk of developing liver disease is small but regular checkups should continue. HBV reactivation is always a possibility but a healthy lifestyle can reduce this risk.
You are correct about the increased risk of liver disease in genotype D patients but even if you had genotype D, your very low viral loads make this a non issue.
Therapy is not necessary to consider right now but please keep seeing your doctor for regular checkups.
1 Like